MLC disease
Article reviewed by Prof. Raul Estevez
Megalencephalic leukoencephalopathy with subcortical cysts (MLC) is a member of the family of leukodystrophies. It is an extremely rare genetic disease. Its frequency is less than 1 per 1,000,000 births, but the disease is more common in certain populations with high consanguinity. It is an orphan disease, which means that there is currently no treatment.
Megalencephalic leukoencephalopathy with subcortical cysts occurs mainly before the age of three and leads to severe neurological dysfunction affecting motor and cognitive functions, which may lead to death. The disease is characterised by infant macrocephaly[1], often associated with initially mild neurological signs (such as mild motor retardation), which worsen over time, leading to difficulty walking, falls, ataxia[2], spasticity[3], progressive seizures and cognitive decline.
[1] Macrocephaly: abnormal increase in the size of the head.
[2] Ataxia: fine coordination disorder affecting voluntary movements
[3] Spasticity: intermittent or sustained involuntary activation of muscles, manifested by muscle stiffness.
Genetic mutation
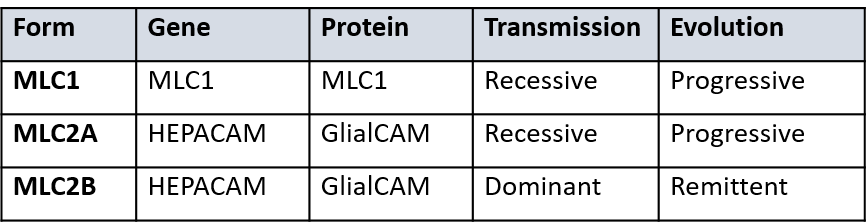
The genes whose mutation is responsible for Megalencephalic Leukoencephalopathy with subcortical cysts are the MLC1gene which is located on chromosome 22 (at 22q13.33) and the MLC2 gene on chromosome 11 (at 11q24.2). Mutations in the MLC1 gene are recessive and are present in 75% of patients. Mutations in the MLC2 gene are recessive or dominant and represent 20% of cases. More than 20 different mutations have been identified in this second gene and doctors distinguish between two forms, 2A and 2B, in these patients. In the MLC2B form, signs and symptoms improve over time, but the reasons for this are not yet understood.
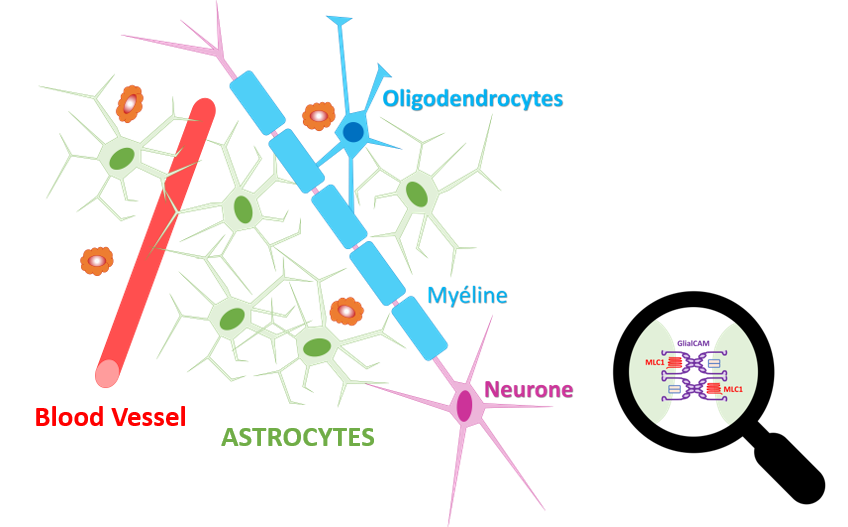
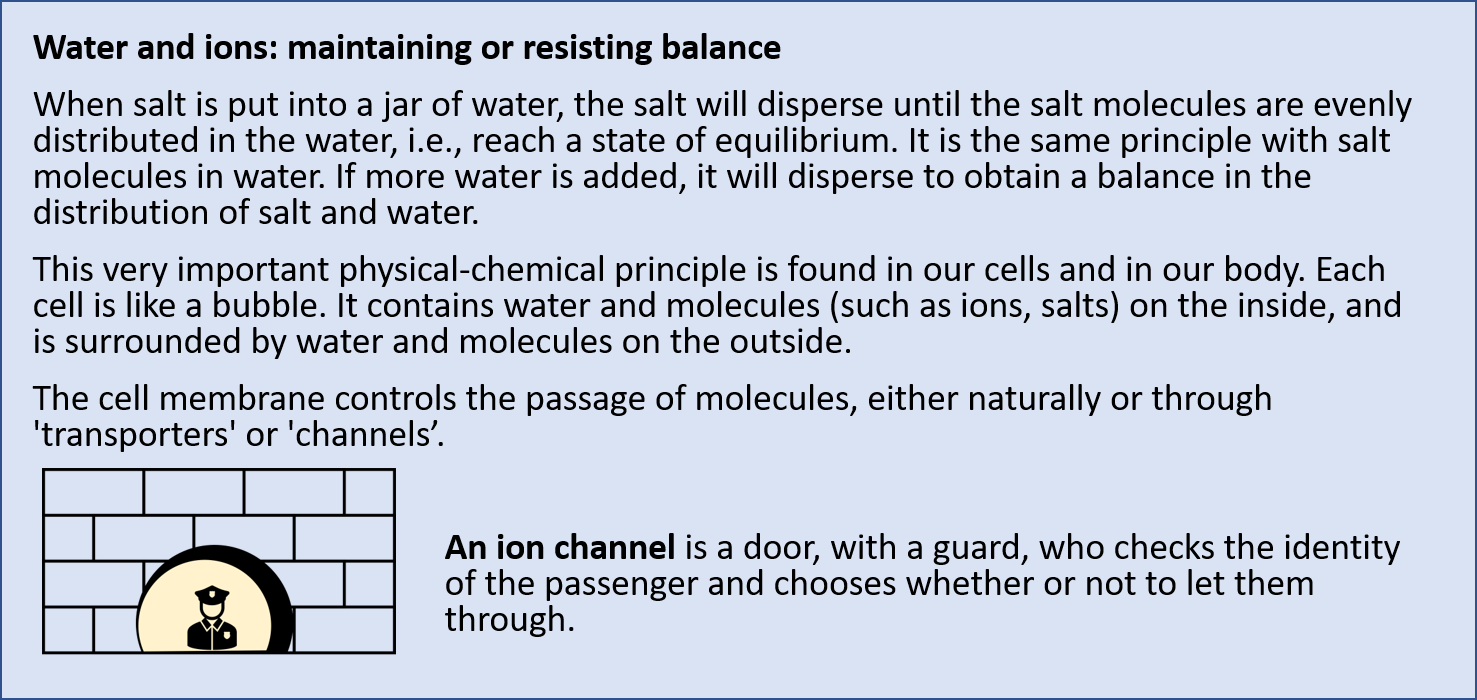
The MLC1 gene codes for a membrane protein of the same name, which resembles an ion channel[1]. The exact function of this protein has not yet been established. MLC2, also known as HEPACAM, codes for an adhesion molecule called GlialCAM. GlialCAM is a better known protein than MLC1. It regulates the localisation of the ClC-2 chloride channel with which it is associated, the localisation of connexin 43, and the maintenance at cell-cell junctions.
Together, the MLC1 and GlialCAM proteins form a complex the function of which is still unknown, but which is mainly produced in the white matter cells that surround the blood vessels, the astrocytes.
[1] Ion channel: a structure in the cell that allows ions to pass in and out. Calcium, potassium or sodium, for example, enter and leave the cells via this type of channel.
Symptoms of the disease
Megalencephalic leukoencephalopathy with subcortical cysts is characterised by progressive motor and cognitive deficits. It is an inherited childhood disease characterised by early onset macrocephaly.
Clinically, patients show deterioration of motor functions with ataxia and spasticity, seizures and mental decline. Unlike other leukodystrophies, megalencephalic leukoencephalopathy with subcortical cysts progresses very slowly, but minor head trauma and common infections can exacerbate the clinical condition of patients.
Many factors seem to be involved in the severity of the disease. Indeed, siblings with the same mutation may have different phenotypes, i.e., express the disease differently. Thus, patients with a clinical picture similar to others at the outset show improvement or even normalisation on subsequent MRIs. This course of the disease corresponds to the so-called MLC2B phenotype. These patients may also have different phenotypes, ranging from a benign transient form of megalencephalic leukoencephalopathy with subcortical cysts, to a form with macrocephaly and mental retardation, with or without autism.
Diagnosis of the disease
When suspected, magnetic resonance imaging (MRI) is used to diagnose the disease in children. Diffuse white matter abnormalities of the brain with mild oedema are visible, as well as subcortical cysts in the frontoparietal and anterior temporal regions.
On a brain MRI, brain white matter swelling with the presence of subcortical cysts and myelin vacuoles, mainly in the anterior temporal regions, are indicative of megalencephalic leukoencephalopathy with subcortical cysts. The diagnosis can often be confirmed by genetic testing of a blood sample. But these tests may also be inconclusive because other genes that have not been associated with the disease are probably involved.
Genetic counselling
In the majority of cases, this genetic disease is transmitted in an autosomal recessive manner, i.e., both parents are carriers of a mutation. The presence of two mutated copies of the gene is necessary for the disease to manifest itself as an MLC1 or MLC2A form. For MLC2B forms, unlike the other two forms, the transmission of the disease is dominant. A genetic counsellor can be consulted to determine the risk of transmission to children. For recessive forms, each pregnancy carries a 25% chance that the child will be affected, and a 75% chance that the child will not be affected.
The simplified mechanism leading to the disease
Megalencephalic leukoencephalopathy with subcortical cysts is an astrocyte disease.
The astrocyte: a key player in white matter
Astrocytes are the most numerous cells in the central nervous system. Thanks to their extensions, they form a complex network of cells. The astrocytes are connected to each other and to the cells of blood vessels (at the blood-brain barrier). Cells exchange ions, small molecules and metabolites via tight junctions. Tight junctions allow for coordinated action by all actors in the network, who then act in unison.
The complex formed by the MLC1 and GlialCAM proteins in astrocytes could modify the functional properties of certain channels responsible for the passage of ions and other molecules, notably across the blood-brain barrier, the border between the brain and the blood. The deregulation of the channels could explain the formation of the vesicles, visible as cysts on MRI, and classifies megalencephalic leukoencephalopathy with subcortical cysts among the so-called cavitary leukodystrophies.
The fact that patients with megalencephalic leukoencephalopathy with subcortical cysts can present with epilepsy is not typical for leukodystrophies, but it is typical for diseases caused by mutations in ion channel proteins. MLC1 could be an ion sensor or a tetraspanin involved in regulating the activity of different proteins through changes in signal transduction. It is envisaged by experts that intracellular calcium dynamics are defective in patients and that this contributes to the pathogenesis.
Day-to-day management of the disease
The treatment of megalencephalic leukoencephalopathy with subcortical cysts is currently supportive symptomatic treatment. Management is based on physiotherapy, psychomotor stimulation and treatment of seizures. It is always possible to offer a comfort solution and all those involved in care, the medical profession and relatives, must work together to identify obstacles and propose solutions.
Treatment research
To date, there is no definitive therapy for megalencephalic leukoencephalopathy with subcortical cysts. A lack of in-depth understanding of the molecular mechanisms of the disease is hampering therapeutic development for this leukodystrophy.
The two main proteins involved in the disease are known, but the function of the MLC1/GlialCAM complex and the associated pathological mechanisms are still unknown. It has been hypothesised that in megalencephalic leukoencephalopathy with subcortical cysts, the role of glial cells in brain ion homeostasis is altered under physiological and inflammatory conditions, explaining the progression of the disease during minor head trauma or common infections.
However, as patients with the MLC2B form have a reversible phenotype, experts envisage that the phenotype of MLC1 and MLC2A patients could also be alleviated by reintroducing the corrected gene, even at later stages. Pre-clinical work supported by ELA is underway to assess the feasibility of gene therapy. Progress is being made in the search for a treatment for megalencephalic leukoencephalopathy with subcortical cysts but there is still a long way to go.